

Why might a horse become weak, wobbly or unable to stand? Dr Philip Ivens MRCVS discusses potential causes
ATAXIA refers to incoordination, which can affect one or more of the limbs and also the neck and body. While this complex condition can result from problems with the vestibular apparatus in the inner ear, or in a part of the brain called the cerebellum, ataxia often arises due to an issue in the spinal cord.
Spinal ataxia occurs when there is a lack of information coming up the horse’s spinal cord to tell his brain where his body parts are in space, and the state of muscle contraction at any one time. Ataxia is therefore not painful for the horse; rather, he has no sense of the position and movement of affected areas.
The hallmark of ataxia is inconsistency. Most orthopaedic lamenesses are consistently repeatable in any one gait, or on a particular surface, but with ataxia the gait changes all the time. A leg might swing out to the side or under the body; a joint might overflex, or a foot scuff or drag.
If he trips, an ataxic horse may be slow to correct himself and potentially fall. His trunk, neck or both might sway. He may tread on himself, or struggle to turn – or instead of crossing his legs underneath as he does turn, he stays rooted to the spot, pivoting while his legs eventually catch up.
A grading system can document the severity of the problem, starting with a zero for normal strength and coordination. Grade one applies to a horse who walks normally in a straight line, but shows a slight deficit when walking on tight circles or with his head extended. He may also sway when pulled by the tail.
A mild increase in muscle tone or weakness in all four limbs, with ataxia at all times – especially during the manipulations mentioned – is graded two, while grade three denotes a more marked increase in stiffness and obvious ataxia, with a tendency to buckle and fall while being circled vigorously, backed up or swayed. A grade four case will spontaneously trip, stumble and fall; at grade five, the horse is recumbent and unable to stand.

SIGNAL PROBLEMS
CERTAIN developmental conditions present at birth can cause ataxia. These include abnormal underdevelopment of the cerebellum, called cerebellar abiotrophy, and abnormal formation of the first and second cervical vertebrae, termed atlantoaxial malformation.
The degenerative condition cervical vertebral malformation (CVM), or wobblers syndrome, leads to compression of the spinal cord and inhibits its ability to carry messages to the brain. And synovial cysts, vertebral fracture and different types of tumour – melanoma, plasma cell myeloma and lymphoma – can press on the nerves and spinal cord.
Infectious disease can result in ataxia: viruses, such as the equine herpes virus-1 (EHV-1, see box), which is endemic in the UK, and the exotic disease West Nile virus, which is becoming established in central Europe and likely to come to the UK at some point. Bacterial meningitis, diseases caused by protozoa – seen mainly in north America – and parasitic causes have also been documented.
Ataxia can be caused by a long list of toxins, the most common of which in the UK is severe nettle rash. Heavy metals such as lead and arsenic may be to blame, or certain therapeutic drugs if used inappropriately – ionophores, for example, such as monensin, found in cattle and poultry feed.
Reaching a diagnosis begins with consideration of the horse’s age and breed and a thorough examination of his history. Has he fallen, for example, or are there stinging nettles in his field?
A routine examination will assess factors such as heart rate, respiratory rate and temperature, to identify any other physical abnormalities that may contribute to or be part of the neurological problem. For example, it is possible for a horse with a foot abscess to look ataxic or for primary muscle disease to cause weakness and similar signs. Perhaps other body systems are involved, such as the skin. If fever is present, an infectious cause becomes more likely.
A neurological examination then follows, comprising tests to identify the part of the nervous system that is affected. This process, neurolocalisation, is a key part of pinpointing the cause and is used to determine whether the spinal cord alone is involved, or if the brain and the peripheral nerves are also implicated. The disease may be focal – centred in one location – or multifocal, affecting multiple places.
Based on these findings, auxiliary diagnostic tests may include a blood cell count, with serum biochemistry, to look for signs of inflammation and other body system involvement. Diagnostic imaging is becoming increasingly helpful; the quality of X-rays of the neck has improved, while advanced techniques such as computed tomography (CT) and magnetic resonance imaging (MRI) are feasible for at least part of the top of the neck.
Sampling the cerebral spinal fluid, either at the atlanto-occipital joint (just behind the ears) or in the lumbosacral area (behind the saddle), is possible and in some cases helpful.

Cerebral spinal fluid is collected under general anaesthesia

The yellowing of fluid is seen in cases of EHM (see box, below)

Radio-opaque dye detects narrowing of the spinal cord
RECOVERY CHANCES
THE prognosis for ataxia is variable, depending on the diagnosis. Stinging nettle-induced ataxia can resolve quickly and fully once the horse is removed from the nettles, sedated and provided with appropriate anti-inflammatories. Sadly, many conditions affecting the spinal cord have a guarded to poor prognosis, due in part to a horse’s size and the safety concerns regarding him and his handlers.
Treatments, including surgery, are improving all the time. When compared with humans and
small animals such as dogs, however, the number of affected horses that can be sufficiently improved to be considered safe is still relatively small.
Repeated neurological examination and diagnostic tests can aid and guide decision-making, ensuring that equine welfare is always put first.
Suspended animation
DISTRESSING images and footage of horses affected by the recent outbreak of EHV-1 in Europe illustrate the neurological effects of this highly contagious disease. The paralytic form, termed equine herpes myeloencephalopathy (EHM), can cause progressive ataxia with marked incoordination of the hind- and occasionally forelimbs, weakness of the bladder and tail, and recumbency.
The virus enters the bloodstream in the immune cells – white blood cells called lymphocytes and monocytes – and is carried around the body. This disseminates the infection to secondary sites, where the virus can replicate in the endothelial cells lining the small blood vessels, which results in infection, inflammation and blood clots. This compromises the spinal blood supply and causes the neurons (nerve cells) to swell and bleed. The extent and location of the neurological lesions determines the nature and severity of the clinical signs.
Modern treatments are available but can be very expensive when dosed for an average-sized 500kg horse. While medications can help, many horses with EHM will die or be euthanased due to complications – often within 48 hours of showing the first clinical signs.
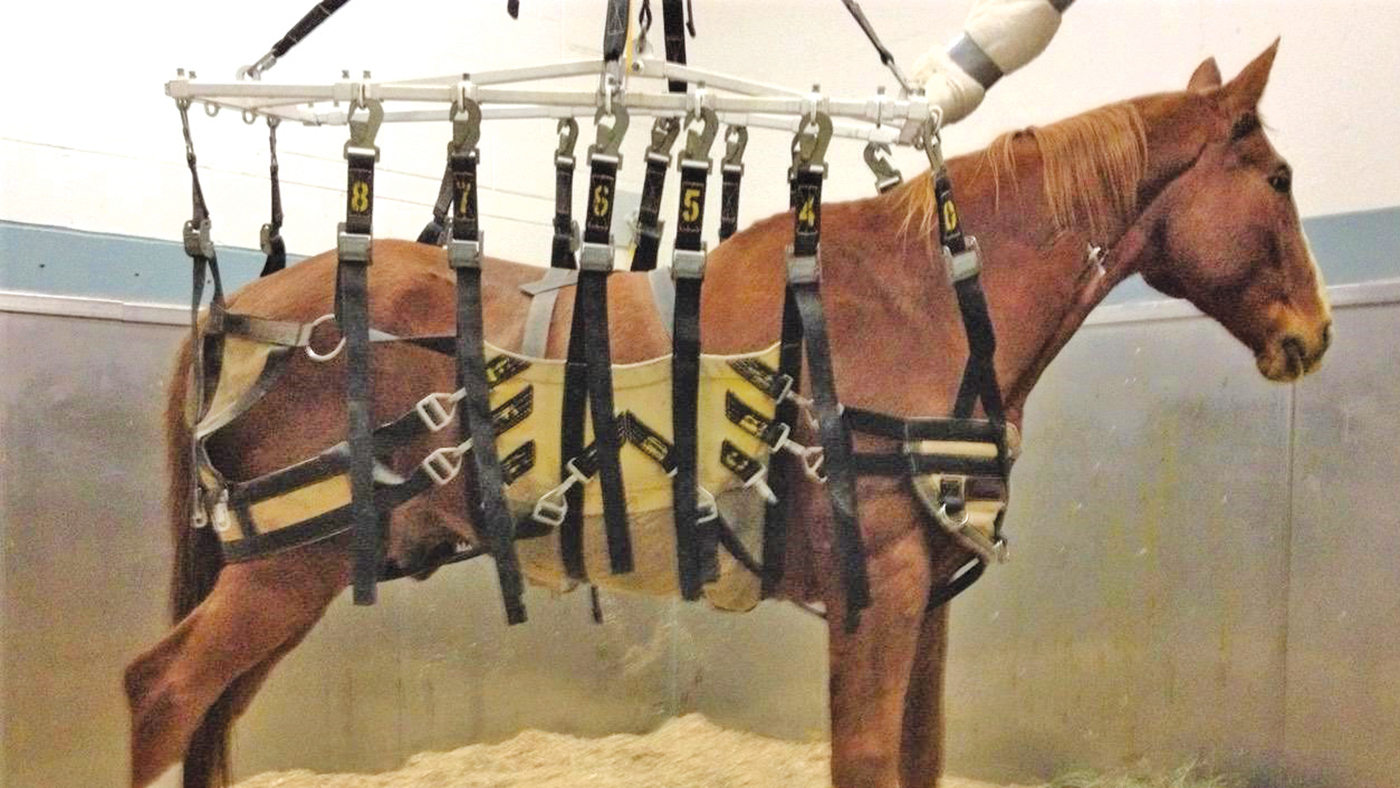
Horses cope poorly with extended time lying down, mainly due to their size, so those that are recumbent are prone to problems including bacterial pneumonia, bacterial cystitis and myopathy (muscle disease). Suspending a horse in a sling during recovery (pictured, above), where possible, can lessen the chance of these complications.
This feature is also available to read in this Thursday’s H&H magazine (15 April, 2021)
You may also be interested in…

Inside the stifle: explaining injuries in horses within this joint *H&H Plus*

Focus on fluids: how to rehydrate a sick horse *H&H Plus*

The dangers of overreach and strike injuries *H&H Plus*
Sharp contact between a hind hoof and a foreleg can cause significant injury, as Dr David Stack MRCVS explains

Calling the vet out of hours: what you need to know *H&H Plus*